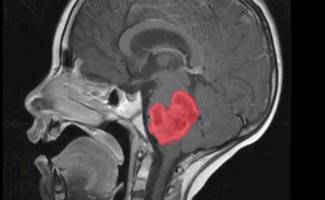
If your child is diagnosed with a DIPG, having surgery to remove the tumour is not a viable option due to the dangers of operating on critical areas of the brain. rarely portions of the tumour may grow outside the brain stem and can be removed.
The standard of treatment for DIPG is radiotherapy, which is usually administered over 3 to 6 weeks depending on the type of radiotherapy that is deemed best for your child (with a daily dose given Monday to Friday). Your child might also be given steroids (Dexamethasone) during this period to help reduce some of the pressure caused by the tumour and radiation treatment. These unfortunately have some very unpleasant side effects but are necessary. This is considered 'palliative' radiotherapy to manage symptoms and is in no way curative.
If hydrocephalus ( a build-up of fluid on the brain.. excess fluid increases pressure which can damage it) is found in diagnostic scans or subsequent scans it can usually be treated using a shunt, a thin tube that's surgically implanted in the brain and drains away the excess fluid. An endoscopic third ventriculostomy (ETV) can sometimes be used as an alternative to shunt surgery. During this procedure, a hole is made in the floor of the brain to allow the trapped CSF to escape to the surface, where it can be absorbed.
Based on the findings of numerous research studies, no single chemotherapy drug has been shown to be effective in treating DIPG, so your child should be unlikely to receive an oral chemotherapy treatment, unless as part of a clinical trial.
This remains to be substantiated with new drug delivery methods (such as convection enhanced delivery) where agents can be delivered directly to the tumour site and by-passing the blood brain barrier. Much more pre-clinical validation with numerous agents and combination studies for best efficacy are needed.
Given the relative lack of treatment options for DIPG in the UK, you may want to consider looking for any available clinical trials, sadly 'in-country' there are very few open trials on offer . In the UK newly diagnosed patients may have access to biopsy profiling and can discuss any options with their oncologist. Many more are available overseas along with self-pay options in private clinics but with stringent eligibility criteria.
Abbie's Army is funding research into DIPG, to unravel the biological landscape and reveal new targets in the treatment of DIPG disease.
Please see our 'FAQ section regarding biopsy procedures...this is not 'standard treatment' for DIPG.
What is the prognosis for DIPGs?
Unfortunately there is NO cure for DIPG at present.
Progression
Although 75- 85% of patients show some improvement in their symptoms after radiation therapy, DIPGs almost always begin to grow again (called recurrence, relapse, or progression). Clinical trials have reported that the median time between radiation therapy treatment and progression is 5-8.8 months.
Any treatment is usually supportive, and palliative relieving the symptoms demonstrated.Unfortunately, DIPGs that progress usually grow quickly and affect important parts of the brain. Clinical trials have reported that the median time from tumour progression to death is usually very short, between 1 and 4.5 months
There are dire statistics for average survival currently , but every child is different. If your child has been diagnosed with a DIPG, focusing on their well being and quality of life is by far the most important thing.