Abbie's Army is proud to be playing it's own small but very important part, in providing much needed strategic investment into DIPG/DMG research. Since the inception of the charity towards the end of 2012 EVERY penny raised has been committed to funding numerous research projects that fulfill our criteria, and have advanced understanding in the field.
There is still much to do, as we begin to see further development of the recent advancements being made between new technologies and drug delivery of agents directly to the tumour site of DIPG . This coupled with a 'combined attack' of other therapy options e.g immunotherapies will become increasingly synergistic with research knowledge.
Bringing these together into relevant trials will be key to success and life extension, if not cure of DIPG in the future.
NEW GD2 CAR-T Cell Therapy Clinical Trial
NEW Grant Award GD2 CAR T Cell Therapy Clinical Trial - £275,000 to GOSH Children's Hospital Charity - Aug 2022
In a first ‘in-child’ use for brain tumours in the UK, 12 children will soon be able to access a new clinical trial using CAR T-cell therapy for DIPG/DMG brain cancers.
Following the release of early data and encouraging results from a US clinical study taking place at Stanford University, a total award of just over £1.2m will go to a team of researchers at University College London (UCL) and Great Ormond Street Hospital (GOSH).
Lead Investigators Dr Karin Straathof and Prof Darren Hargrave will utilise a ‘GD2-CAR’ as previously used in the UK in clinical trials for the children’s cancer neuroblastoma. Patients will be treated by an expert multi-disciplinary team at Great Ormond Street Hospital (GOSH) but will be referred from throughout the UK to take part in the clinical trial.
Abbie’s Army have been instrumental in the provision of funding for the trial.
Using our position within the childhood cancer community the charity has made a collaborative grant award of £275,000 to Great Ormond Street Hospital Children’s Charity (GOSH Charity). We were also able to direct further funding from The Azaylia Foundation and CRIS Cancer Foundation towards the study.
We are incredibly grateful for their interest and willingness to help to support the trial.
Driven by research funding from Abbie’s Army the direct amount funded includes support from six other parent-led charities: Islastones Foundation, Bradley Lowery Foundation (including Kaleigh’s Trust and The Spider Ede Appeal- DIPG Awareness), Robert Andrew Munro Foundation, Eva’s Angels, Doing It For Daniel and Edie’s Kindness Project.
Speaking on behalf of Abbie’s Army Amanda Mifsud said, “I’m overwhelmed at the response from our own DIPG/DMG ‘community’ joining us to fund collaboratively and support this new innovative clinical trial. All family groups know how precious some ‘hope’ can be and it means everything to them to provide other families with opportunities previously unavailable to them, in memory of their own children”
We're grateful to GOSH Children’s Charity who coordinated funding between Abbie’s Army and the other main funding groups involved.
Principal investigators:
Dr Karin Straathof, Associate Professor at the UCL Cancer Institute and Honorary Consultant at GOSH.
Prof Darren Hargrave, GOSH Charity Clinical Professor in Paediatric Neuro-Oncology and Honorary Consultant at GOSH.)
Phase 1 Clinical Trial of GD2 CAR-T cells for 12 patients: £1.2 million
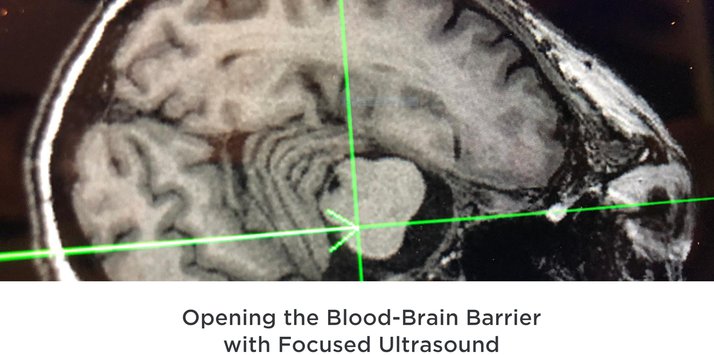
Bringing Focused Ultrasound (FUS) to clinical trial readiness
Dr Antonios Pouliopoulos - 'Focused Ultrasound for targeted carboplatin delivery in DIPG’ - King’s College London, £10,000 April - September 2022.
In November we partnered with the CBTDDC (Children's Brain Tumour Drug Delivery Consortium) to offer an award of £10,000 as part of their 'clinical trial readiness pump prime funding call'. The successful project was selected with support of their scientific advisory panel to enable a new clinical trial research proposal to move another stage forward for DIPG/DMG children in the UK.
Now a team lead by Dr Antonios Pouliopoulos of King’s College London, with collaborators from Great Ormond Street Hospital for Children are investigating how to effectively and safely deliver chemotherapy to children using ‘Focused Ultrasound for targeted carboplatin delivery in DIPG’
The new focused ultrasound technique works to temporarily open the blood-brain barrier, the natural protective layer in our brain which is essential for normal brain function, but also limits the ability of any systemic medications like chemotherapy from reaching the site of DIPG disease and other brain tumours.
The technology uses focused ultrasound and microbubbles—gas-filled contrast agents used for imaging and drug delivery—coupled with real-time neuro-navigation guidance for the treatment of brain diseases. Given intravenously, the liquid-coated microbubbles travel to the treatment site. The gas inside these tiny bubbles vibrates once the ultrasound beam shines on them, and causes cells to pull apart providing temporary access to the brain.
If the procedure can be done safely, we can potentially use medicines at lower concentrations reducing toxicity and side effects for children undergoing treatment.
Dr Pouliopoulos also maintains a key role in the team at Columbia University NY who are currently running a focused ultrasound clinical trial (NCT04804709) for DIPG patients, using precisely the same focused ultrasound technology developed to increase drug delivery.
His involvement and published pre-clinical studies were pivotal in propelling this technology forward for approval for use in DIPG and there is a wealth of experience within the team at King’s College London in drafting the necessary regulatory requirements, for use in the UK.
Photo credit ‘Pouliopoulos et al, 2020, Ultrasound in Medicine & Biology 46,1’
Totally non-invasive, for children enrolled in the US trial the entire treatment session per patient currently lasts only 20 to 30 minutes and occurs three times a week over six bi-weekly cycles in the current trial.
The treatment is painless, simple and quick, and so can easily be repeated multiple times a week, if required by the dosing of the drug.
The tumour is first targeted by focused ultrasound to achieve blood-brain barrier opening after intravenous administration of microbubbles, and subsequently is followed by the intravenous or oral administration of the drug.
This is a huge benefit for families who obviously want to subject their children to as little as possible, as a fully portable, small-scale system like this also provides numerous other advantages in terms of hardware costs and potential accessibility at treating centres.
Your support crucially will finalise the information needed to complement existing data from 5 years of previous research and development, providing the evidence to show that BBB penetration of carboplatin can be enhanced with FUS.
A successful MHRA application to trial in the UK should be ready by the end of September 2022, and after approval a clinical trial is planned to start in 2023.
Dr Karin Straathof - Multi- modular IL13RA2 CAR T cell therapy for Diffuse Midline Glioma' - UCL Great Ormond Street Institute of Child Health - £477,016.58 Jan 2021
Abbie's Army is pleased to announce that we have finalised the agreement of a brand new grant to enable the opening of a clinical trial using CAR-T cell therapy.
Principal Investigators are: Dr Karin Straathof, UCL Great Ormond Street Institute of Child Health, Dr Martin Pule - Lead of the UCL CAR-T Cell Programme, Dr Aquilina, neurosurgery clinical lead at Great Ormond Street Hospital, Dr Darren Hargrave, Paediatric Neuro oncologist, Great Ormond Street Hospital
The study is anticipated to open 2023, we have co-funded the trial based on evaluation and joint monitoring of study milestones and first funding instalments commenced on January 1st 2021.
This clinical trial will offer 12 children in the UK, with a diagnosis of DMG/DIPG to have the same opportunities as children in the United States who have access to these most recent innovative studies. (Trials using GD2 and B7-H3 targets have just begun in the US)
This clinical trial utilises CAR-T cell therapy targeting the antigen IL13-RA2.
The development of this treatment approach has identified a marker or 'antigen' IL13-RA2 (Interleukin 13 Receptor Subunit Alpha 2) a protein coding gene on the outside of DIPG tumour cells that is absent on healthy cells; this allows the building of a CAR (chimeric antigen receptor) which tells the T-cells to recognise that marker on a cancer cell.
Our study in DIPG is a 'second generation' or 'multi modular' CAR which has now been developed for clinical trial patients in the UK. It will have FOUR functions.
* Tracking to the DIPG tumour antigen marker IL13-RA2 - designated as "A2R72 CAR-T cells"
* Priming of the DIPG tumour micro-environment to make the treatment more effective . DIPG's surround themselves in an immunosuppressive environment, a genetic module will make T cells resistant to these conditions.
* Additional module for 'cytokine IL-15' production that maintains CAR longevity in the body
* A 'suicide switch' so that if necessary the effects of the CAR can be turned 'off'
We re indebted and grateful to our donors and incredible partner DIPG families that have contributed and allow us to contribute to this vital work.
The trial will inform the basis for further development of the CAR-T program in the UK for all patients with DIPG/DMG in the future.
Development of H19-targeting antisense oligonucleotides for DIPG therapy
Dr Francesco Crea - Development of H19-targeting antisense oligonucleotides for DIPG therapy - The Open University - December 2019
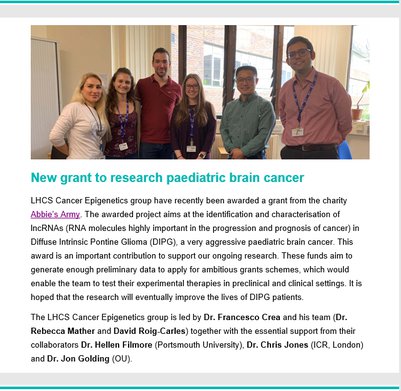
Your invaluable support has enabled Abbie's Army to award a grant to Dr Francesco Crea and his cancer epigenetics team at the The Open University Titled “Development of H19-targeting antisense oligonucleotides for DIPG therapy” this collaborative project also includes Dr Helen Fillmore from the University of Portsmouth , Prof Chris Jones of The Institute of Cancer Research and Dr Jon Golding also of the OU.
The most frequent mutation in DIPG occurs at histone H3 lysine 27 (H3K27M) resulting in widespread epigenetic dysregulation, despite global efforts no effective protein-targeting therapy has been developed for DIPG. Long noncoding RNAs (lncRNAs) are non-protein coding transcripts, for several decades, lncRNAs have been considered non-functional transcriptional noise, more recently however numerous lncRNAs have emerged as important regulators of many biological processes. Sequencing data has revealed they represent a vast and largely uncharted region of the human transcriptome (more than 50,000 unique loci, <2% of which has been characterised). In addition, research already conducted by the team and by other groups has identified specific lncRNAs as drivers of cancer cell drug resistance, migration and invasion. For these reasons, lncRNAs could also be considered a potential ‘gold mine’ for discovery of new biomarkers and therapeutic targets in oncology.
Antisense oligonucleotides (ASOs) are short DNA strands that bind specific RNA targets and trigger their degradation. The preferred route for ASO delivery to the central nervous system (CNS) is by intrathecal injection which results in high cerebrospinal fluid concentrations, broad distribution in the CNS and rapid cellular uptake of ASOs. Here the team are proposing to develop lncRNA-targeting ASOs to stop DIPG proliferation, with the final goal of developing personalised therapies for this incurable disease. Based on the teams preliminary data the most up-regulated transcript found in DIPG is the embryonal lncRNA 'H19', confirmed in samples versus other paediatric gliomas and normal developing brain, it is also significantly associated with H3K27M mutation. Since lncRNA’s can be targeted with antisense therapy several H19 targeted ASO’s have already been designed and tested by the group. One clearly induced a dose and time dependent inhibition in DIPG growth confirming it as a potential therapeutic target in the disease.
The grant will cover further validation in DIPG cell lines, clarification on the mechanism of action, as well as the role of H19 in connected radio sensitivity ‘silencing’ in DIPG cells. We look forward to bringing you further updates during this interesting novel study.
Dr Helen Fillmore - 'Key signalling pathways in the micro-environmental landscape of the developing pons and DIPG' - University of Portsmouth - £43,159 Feb 2019
This will be addressing some of the significant gaps in the understanding of the influence of tumour microenvironment and brainstem development continuing collaborations preparing potential target areas for further investigation. The fact that DIPG arises in a region and age specific nature strongly supports the suggestion of dysregulation in a postnatal neurodevelopmental process. Key research questions focused on understanding how tumour micro-environmental elements (TME) affect tumour biology and therefore any responses to treatment will be crucial to progress. If we are to have better understanding of the origins of DIPG, precisely what controls the ‘evolution’ of disease and the maintenance of those malignant tissues, we may learn how to reverse or restore early key regulatory signalling pathways.
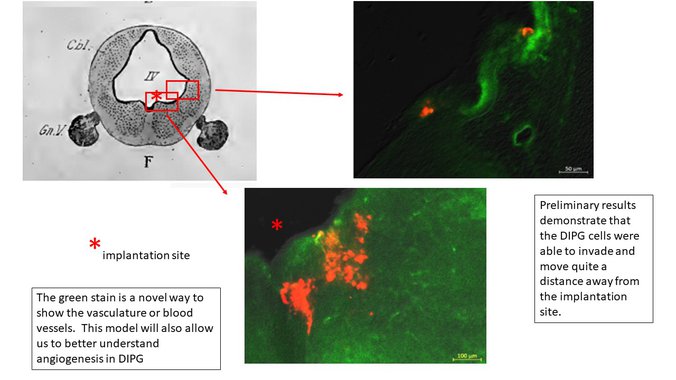
The ‘TME’ is only one part of a DIPG treatment strategy as much as treating the ‘downstream’ molecular changes themselves as disease resistance develops and tumour cells carrying a particular ‘target’ vary during its course. The funding also includes exciting work to validate and develop new pre-clinical chick embryo models for DIPG. (Unpublished pictures below with permission from Dr Frank Schubert and Hanna Russell - notice the ability of DIPG to migrate away from the implantation site!!!)
The brainstem developmental time frame for chicks is similar to humans, especially in terms of the pons area. This is a unique opportunity to develop a model which will enable identification of key cell to cell interactions that are involved in driving tumour growth. During the grant Dr Fillmore will also continue the mentoring of a very talented pre-doctoral student, Katie Loveson working currently on the roles of tumour cell proteins and validation of deferentially expressed extracellular matrix molecules in DIPG.
DIPG Trials Researcher - Institute of Cancer Research - 2 Years £73,000 - Feb 2019
Abbie’s Army has been supporting Professor Chris Jones’ laboratory for some time at the Institute of Cancer Research. We have been funding processing and analysis of DIPG samples for children enroled on the UK BIOMEDE trial for DIPG, we have funded the molecular profiling and modelling of 40 patients enrolled.
However, we now need to do MORE to progress this research.
Professor Jones’ laboratory is becoming the UK biology reference centre for more DIPG trials, and so there is need to fund a dedicated DIPG Trials Scientific Officer within the team and to expand ICR’s capacity, this will continue the work not only on the BIOMEDE samples, but include children’s samples from other trials in the UK and Europe.
Elisabet Fernandez Potente has now been selected by Professor Jones to join the team.
Abbie’s Army is working alongside the 'Islastones' group based in Hinckley who want to fund this new researcher who will process the trial samples and attempt to establish both 2D and 3D cell cultures in the laboratory. They will ensure the models undergo molecular profiling and carry out bespoke drug screening needed to inform the treating clinicians of children enrolled.
By supporting this research you will be playing a major part in efforts to develop tailored treatments for children with DIPG, in the fastest possible time, with maximum benefit and minimum side-effects. A targeted treatment is also a ‘kinder’ treatment.
Abbie’s Army will still be funding all the biology for all trials for each patient investigated. Funds are still needed to cover the position for two years but the urgency of the situation has necessitated this appointment right now.
PDX 'Avatar' Analysis for BIOMEDE 2017 (Ongoing)
Professor Chris Jones - PDX 'Avatar' Analysis for BIOMEDE 2017 - Institute of Cancer Research, Sutton - £100,000
During the end of 2016 we expressed an interest in working alongside The Institute of Cancer Research and Prof Chris Jones - a previous recipient of Abbie's Army funding , on a much broader analysis of the biopsy samples taken for those enrolled on the UK trial known as BIOMEDE.
This is the only 'adaptive' clinical trial currently open in the UK and involves upfront biopsy and stratification of patients to various treatment arms of the trial dependent upon their genetic mutation. This determines which drug they will initially receive, and so most importantly for the first time they will be trialed against a target they know is actually 'present' At the same time a key feature of the BIOMEDE trial is the introduction of experimental agents should an appropriate 'target' be found during the molecular analysis and broader sequencing of the individual child's tumour.
To build on this feature, we have pledged funding on a 'per patient' basis to establish 'Patient Derived Xenografts' or PDX models (also know as avatars) of individual patient disease for screening and testing in vitro and vivo . The most efficacious agents identified will be fed back to the treating clinicians in the individual patients treatment centre.
This is a huge challenge but biopsy has a hugely important role to play, indeed throughout the evolution of DIPG disease as it adapts to single agent therapy and creates resistance.
It is hoped this study can highlight the most effective combinational therapies as well as validate the clinical use of PDX models in DIPG treatment. All data will also be fed back to Registry sites.
Abbie's Army has initially limited this funding to £100,000 and will review it's potential with the results from sampling obtained.
Targeting BDNF- TrkB Signalling & CAR-T Therapy (Immunotherapy) in DIPG
Monje Lab - Towards a multi-pronged approach for DIPG therapy targeting BDNF-TrkB signalling in the DIPG micro environment' - Stanford University $270,000 (£210,000) July 2017-2019
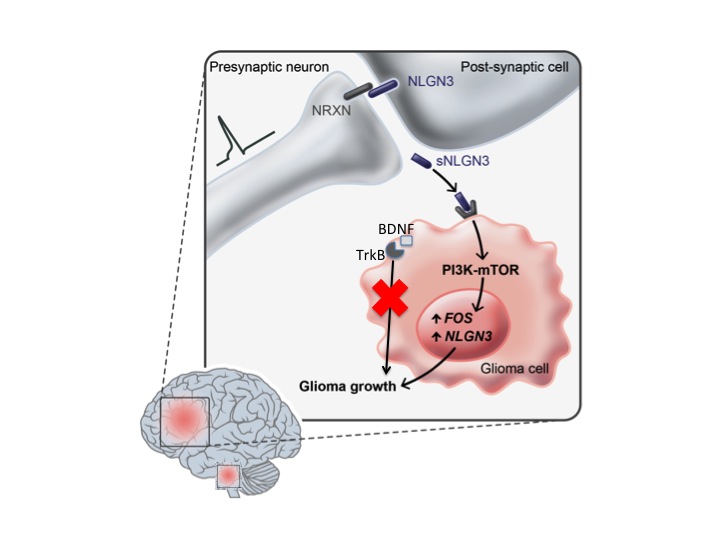
Successful treatment of diffuse intrinsic pontine glioma (DIPG) will likely require a multi-pronged approach, targeting intrinsic vulnerabilities of DIPG cells, blocking key signals from the micro environment of the developing childhood brain that fuel DIPG growth, and directing the immune system to attack the cancer. DIPG hijacks mechanisms of development and plasticity in the childhood brain. Neuronal activity is a key regulator of brain development and plasticity, and the Stanford lab have recently shown that active neurons in the tumour micro environment robustly promote DIPG growth.
A growth factor called “brain-derived neurotrophic factor” (BDNF) is secreted in response to brain activity and plays numerous roles in childhood brain development.
BDNF is also important for the adaptability of the brain necessary for learning and changing in response to experience. We have identified BDNF as a molecule that promotes DIPG proliferation, and hypothesize that DIPG subverts BDNF signaling to promote cancer growth.
In the proposed experiments, we seek to determine the therapeutic potential of blocking BDNF signaling in DIPG, cutting off what we hypothesize is a key micro environmental factor fueling DIPG growth. The majority of the proposal focuses on BDNF, a leading candidate for micro environmental therapy in DIPG.
Parallel work from the Stanford group has also focused on developing an effective immunotherapy strategy for DIPG and included in the proposed project are a discrete set of experiments seeking to advance our mechanistic understanding of a promising immunotherapeutic strategy using chimeric antigen receptor T cells (CAR-T cells).
Ultimately, the goal is to identify and combine optimum therapeutic tergeting involving immunotherapy and more synergistic strategies like targeting the micro environmental determinants of DIPG growth. This sort of “one-two punch” approach, hitting the cancer from different angles, will move us closer towards the goal of defeating DIPG.
Abbie's Army is pleased to announce this grant , which is it's largest so far, after careful review by our scientific advisories and considerable discussions and negotiations with Michelle Monje. The 'can-do' attitude at Stanford is impressive and inspiring as are some of the results being achieved, thus far in unpublished 'data' . In the context of so many other developments coming to fruition here the Trustees felt there is great potential and every reason to be hopeful for the development of an effective combination therapy for DIPG, with a clear path to implementation in clinical trial.
Combined use of CDK4/6 and mTOR inhibitors induce synergistic growth arrest of DIPG
Combined use of CDK4/6 and mTOR inhibitors induce synergistic growth arrest of diffuse intrinsic pontine glioma cells via mutual downregulation of mTORC1 activity
Latest research now published from the University of Bristol Functional Neurosurgery Research Group, lead by Steven Gill We're proud to have funded this study that should add to greater lines of defence for use in future DIPG treatment via CED (convection enhanced delivery) - this fully supports the rationale for inhibition of multiple disease pathways, and the development of much needed optimal combinations of multiple drugs. "Direct infusion of palbociclib into the brain, in combination with systemic delivery of temsirolimus, represents a promising new approach to developing a much-needed treatment for DIPG"
A NEW paper was published today (15th April) in the Journal Nature Medicine from the Monje lab at Stanford University.
'Potent antitumour efficacy of anti-GD2 CAR-T cells in H3 K27M+ diffuse midline gliomas' Funding was contributed by numerous family led foundations including Abbie's Army.
The 'data' is incredible for this new promising immunotherapeutic 'CAR-T cell' approach for DIPG and other diffuse midline tumours. The disease even in the most robust model was eradicated, (do take a look at the luminescence imaging of the models included in the full pdf )
Abbie's Army with your support funded some of the GD2 specificity experiments required to enable publishing on this paper as part of a $270,000 funding award made last Summer. Clinical trials for the CAR-T treatment are planned for Spring 2019 safety will be so important given the precarious nature of the tumour site, monitoring and intensive care of neuroinflammation will be required, but a 'cautious multidisciplinary clinical approach' could prove 'transformative' for patients.
Incredible work, which we are so very proud to support from Michelle Monje-Deisseroth Crystal Mackall and the Stanford team.
Read the full Nature release in 'Recent DIPG Research News'
Panobinostat in PDX Models
Pre-Clinical Study of Panobinostat in Xenograft and Genetically Engineered Murine Diffuse Intrinsic Pontine Glioma Models
This was a collaboratively funded project and Abbie's Army are listed here as a contributor on this release from Oren Becher.
Conclusion
Our collaborative pre-clinical study confirms that panobinostat is an effective targeted agent against DIPG human and murine tumor cells in vitro and in short-term in vivo efficacy studies in mice but does not significantly impact survival of mice bearing H3.3-K27M-mutant tumors. We suggest this may be due to toxicity associated with systemic administration of panobinostat that necessitated dose de-escalation....
In October the charity , co funded with Finlays Fighters continued its support of The Institute of Cancer Research via funding granted through the DIPG Collaborative’s ‘Medical Advisory Council’ for a further years study –
‘The Evolutionary Dynamics of DIPG’ ( $97,470 - £62,169 )
In the first year of this grant, funded by the Abbie’s Army substantial progress was made in ascertaining the sub-clonal architecture of DIPG using next-generating sequencing of single, multi-region and longitudinal samples. Additionally the Institute developed methodology to isolate DIPG subclones in vitro in order to determine how distinct genotypes link to function within the tumour mass. As highlighted in the original application, a second year of funding was requested to more fully explore the interactions between subclonal populations of DIPG cells, and to assess the possibilities of disrupting communication between these subclones as a novel therapeutic strategy.
Bristol Functional Neurosurgery Group
Bristol lab and Dukes University (Oren Becher) - Collaborative study for combinations in CED with carboplatin.
With the emergence of new technologies for drug delivery and the ability to bypass the ‘BBB’ Blood brain barrier, the outlook for the treatment of DIPG and other neurological conditions is changing.
The charity had become aware of several children treated at Bristol Children’s Hospital on a ‘compassionate’ basis with a technique known as convection enhanced delivery or ‘CED’. Crucially the delivery of the most effective targeted agents based on new knowledge of tumour biology will be instrumental to the success of the method, although it is still likely that a combination of agents and treatments will be needed to change this ‘terminal’ diagnosis to chronic.
With this in mind the charity, co-funded with Finlay's Fighters, expressed interest in a collaborative project ;
‘Identifying new drug combinations for the treatment of brainstem tumours in children using a novel method of direct drug infusion into the brain’ - (£72,763)
This was an annual study commencing May 2015 between the ‘Functional Neurosurgery Research Group’ at the University of Bristol and Oren Becher of ‘Dukes University’ North Carolina in the US.
Aim of project
The aim of this project is to identify new drug combinations for the treatment of brainstem tumours in children using a novel method of direct drug infusion into the brain. Suitable drugs will be selected by undertaking a comprehensive programme of pre-clinical research designed to determine whether the selected drugs could be safe and effective.
Background
In Bristol children with progressive brainstem tumours were treated using a novel neurosurgical method of drug delivery to the brain called Convection-enhanced Delivery (CED). The method involves the robotic implantation of very fine catheters into the brain and infusion of drugs directly into the tumour, thus bypassing the BBB. This technique has been found to be safe and to show promising signs of efficacy. Importantly the risk of children suffering intolerable side-effects when chemotherapy is administered by CED is very low.
Project description
This project represents a progression from work completed in the USA by a group dedicated to developing new treatments for children’s brain tumours, as well as our own work in the UK developing novel ways of delivering drugs to the brain. The US group has developed a model of brainstem tumours in mice which closely resembles the human disease both genetically and structurally. This unique model of DIPG offers an opportunity to test drugs targeting specific pathways which are upregulated in the human disease. The complex biology of DIPG means that it is very likely that two or more drugs used in combination are more likely to be effect that any single therapy.
Specifically the project aimed to study the suitability of drugs which act through the following mechanisms: 1. AKT inhibition e.g. perifosine 2. CDK4/6 inhibition e.g. palbociclib 3. mTOR inhibition e.g. temsirolimus, sirolimus or everolimus 4. MEK inhibition e.g. trametinib
The charity received updates on request and upon completion of scheduled calls with the US research team. By the end of the year they were beginning to identify efficacious drug combinations, when delivered using the catheter systems, could make an impact on this devastating disease and inform clinical trial.
Palbociclib has the potential to selectively inhibit the unfettered proliferation of DIPG cancer cells via reestablishing the cyclin D-CDK4/6 regulatory pathway, which curtails cell proliferation at the G1 phase of the cell cycle. It is a FDA approved drug and has shown efficacy in breast cancer to date. Temsirolimus selectively inhibits the kinase, mammalian target of rapamycin m TOR and as a consequence blocks the translation of cell cycle regulatory proteins and prevents the over expression of antigenic growth factors. It is a FDA approved drug, but in its current form it is insoluble and therefore would need encapsulation to be progressed towards the clinical setting. The project began by assessment of the various drugs within the DIPG cell lines, moving forward Duke university concentrated their efforts on Trametnib and Bristol have concentrated all efforts on Palbociclib (CD4/6) and temsirolimus (mTOR inhibition).
The following conclusions were established: - Identification of potential therapeutics which could be effective in DIPG. - Preliminary combinational drug strategies that show efficacy in DIPG cell lines. - Initial assessment of the toxicity of the drugs in-vivo
DIPG Collaborative ( Year 1 )
Evolutionary Dynamics of DIPG ( Year 1 )
The DIPG Collaborative
Late 2013 we made a funding contribution at the required level of investment ($25,000 - £17,800) to become ‘Foundational Leadership Partners’ within a group of primarily US based foundations – The DIPG Collaborative.
The DIPG Collaborative is a collection of foundations with the common interest of inspiring research into the cure of Diffuse Intrinsic Pontine Glioma (DIPG) with the belief that through a cure for DIPG, significant advances in other cancer research will be made.
Today the DIPG Collaborative is made up of nearly 30 foundations that cooperatively fund DIPG research funding every two years. The DIPG Symposium, which occurs every two years, is the culmination of not only the DIPG Collaborative's funding cycle, but also features unique perspectives on research from experts around the globe.
It is a wonderful thing to play a part in having a much wider impact on the disease, all grants funded via this group are ‘peer reviewed’ by their medical advisory council and ranked in order for funding application.
At the end of 2013 collectively the group funded $850,000 of research on 9 projects and Abbies Army via their contribution became listed on all 9 grants as a contributor to this work.
At the same time a funding application was made by Prof Chris Jones at The Institute of Cancer Research via the Collaborative which sought to define the subclonal diversity of DIPG with a view to better understanding the evolutionary dynamics underlying this highly heterogeneous tumour. Ascertaining the subclonal architecture of DIPG will be performed using next-generating sequencing of single,multi-region and longitudinal samples.ICR have additionally developed methodology to isolate DIPG subclones in vitro in order to determine how distinct genotypes link to function within the tumour mass.These interactions between sub clonal populations of DIPG cells need full investigation in order to assess the possibilities of disrupting communication (progression) as a novel therapeutic strategy. Towards the end of 2014 we invested the sum of $115,325( £56,558) sterling equivalent in order to fund this grant application ‘The Evolutionary Dynamics of DIPG’ to run until September 2015.
PhD - Institute of Cancer Research
By funding scientists who have the potential to become leaders in their field, we are not only adding to the headcount of persons working in this underfunded area of medicine, but we are tapping into novel and innovative ideas that hopefully will lead to significant breakthroughs in diagnosis and treatment options in this field.
We want to find and contribute as much as possible to that elusive DIPG CURE!
Kathryn Taylor PhD - The Institute of Cancer Research Award £110,000
Dr Chris Jones appointed, by his peers is the Chair of the SIOPE High Grade Gliomas/DIPG Biology Group (International Society of Paediatric Oncology - Europe) and Principal Investigator (Genomics) on the North American DIPG Collaborative Grant and as such is the international lead on research into these tumours.
Following a visit of Abbie’s Army to the ICR in October 2013, we were presented the following project with the costs required to take forward this research into DIPG over the next two years:
'Translational genomics of diffuse intrinsic pontine glioma'
PhD Studentship – Kathryn Taylor
Project finishing in September 2015
Supervisor: Dr Chris Jones, Institute of Cancer Research, Sutton
The goal of Katy’s project is to identify and test novel therapeutic targets for DIPG. This comprises two main areas of work: Whole genome sequencing of a series of DIPG biopsy specimens Development of novel DIPG models
In the first two years of her project, Katy has successfully completed the biopsy sequencing study, and has a first author paper at Nature Genetics in addition to a second paper, of which she is also a contributing author (see below). Both studies have identified a gene known as ACVR1 as a major new driver in DIPG, with mutations found in approximately 25% of cases. Remarkably, these are the same mutations found in patients with the rare congenital malformation syndrome called fibrodysplasia ossificans progressiva, in which the soft tissue turns to bone. This discovery offers new insight into the links between cancer and development, and provides a new target for novel therapies in DIPG. Katy will continue to work on the functional aspects of ACVR1 in DIPG whilst funding is sought to employ a new post-doctoral fellow to take this project forward. In addition the sequencing study has identified further targets involving cell signalling pathways which also bear investigation.
In parallel, Katy has been attempting to grow numerous DIPG primary patient-derived cell cultures obtained from collaborating centres across the world. She has successfully established 8 DIPG primary cell lines as both two-dimensional stem cell cultures and three-dimensional neurospheres (clusters of cells that more closely replicate a tumour). In addition she has produced tumour models with similar cellular and invasive growth characteristics as the human disease. She is currently in the process of generating molecular profiles of these models, and they will provide the resources for assessing the potential clinical utility for the targets identified from the sequencing of the human DIPG samples.
The first step in bringing these two strands together is to carry out a functional genetic screen on the cell lines. This will include a specific ‘synthetic lethality’ experiment to identify which combination of genetic ‘hit’ selectively kills the mutant ACVR1 cells. Katy will use this information to identify alternative approaches to drugging this pathway which may be quicker to translate to the clinic given the current lack of available drugs that target ACVR1. In addition such a screen can be repurposed towards a comprehensive assessment of all candidates generated from the sequencing study to identify and prioritise the most important for preclinical study. In order to achieve this, we wish to expand the depth and breadth of our original experiment to include the entire ‘druggable genome’ across an expanded panel of DIPG cells. This will generate a unique dataset that to our knowledge is not being undertaken elsewhere.
It is anticipated that such a screen will run in the first 6 months of 2014, providing valuable functional dependency data for the ACVR1 project, and allowing for selection of novel candidates for the remainder of Katy’s PhD. The rest of her time will be spent carrying out detailed investigations for drugs targeting these most promising candidates. Owing to our leadership roles in the European DIPG working group, it is anticipated that the preclinical data generated will be used to guide the next generation of clinical trials currently being designed. Katy is an extremely talented young researcher. Supporting the remainder of her PhD made a significant contribution to the efforts at ICR to come up with better treatments for children with DIPG. Katy also received a prestigious award for her work at the SNO (Society for Neuro Oncology) conference in San Francisco in November 2013.
We were delighted to have been able to support Katy in her studies ...and even more delighted and humbled that Katy dedicated her thesis to Abbie.
Children's Brain Tumour Research Center
Children's Brain Tumour Research Center - Nottingham (2011-2012)
Immediately after Abbie's death we began fundraising in support of the CBTRC at Nottingham.
At the time we set ourselves a very small target, but the outpouring and need for people to make 'sense' of something that made no sense at all, meant that by the time Abbie's funeral came around £12,000 had already been collected.
We donated via JustGiving to the centre in furtherance of all their aims until deciding that the need to become 'DIPG specific' and tackle this cancer that took Abbie's life was important and much needed.
In our first initial months until the diversion a fantastic £82,000 was raised and donated - with just over £15,000 of that also being donated to the Royal Marsden Cancer Charity.

 The new focused ultrasound technique works to temporarily open the blood-brain barrier, the natural protective layer in our brain which is essential for normal brain function, but also limits the ability of any systemic medications like chemotherapy from reaching the site of DIPG disease and other brain tumours.
The new focused ultrasound technique works to temporarily open the blood-brain barrier, the natural protective layer in our brain which is essential for normal brain function, but also limits the ability of any systemic medications like chemotherapy from reaching the site of DIPG disease and other brain tumours.